Posted by On The ROAD To Good Health | Filed under car accident, Uncategorized

20 Tuesday Oct 2015
Posted by On The ROAD To Good Health | Filed under car accident, Uncategorized
20 Tuesday Oct 2015
Posted in car accident, Uncategorized
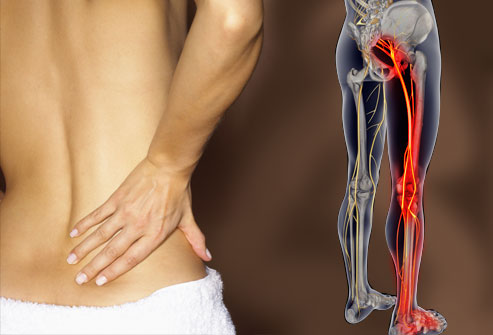
The longest nerve in the body is the sciatic nerve, which runs from the spinal cord to the buttocks and hips, continuing down the back side of each leg. When the sciatic nerve is damaged or injured, sciatica occurs, referring to the pain that is created throughout the entire nerve – from the spinal cord all the way down through both legs.
While sciatica is a medically recognized injury that needs to be treated on its own, it is also a major indicator of a much larger injury that has either taken place in a region of the body that can affect the sciatica, or a major injury could be on the brink of happening in one of these regions. With that, sciatica is both an injury and a symptom, reflective and indicative of problems like a herniated disc or trauma.
Sciatica can be intensely uncomfortable and irritating, causing mild to extreme pains shooting through the length of the body. And while that pain can be agonizing at times, it can sometimes only be treated with time and rest, which means that the discomfort could last as long as two months.
Symptoms
Pain that radiates from your lower (lumbar) spine to your buttock and down the back of your leg is the hallmark of sciatica. You may feel the discomfort almost anywhere along the nerve pathway, but it’s especially likely to follow a path from your low back to your buttock and the back of your thigh and calf.
The pain can vary widely, from a mild ache to a sharp, burning sensation or excruciating discomfort. Sometimes it may feel like a jolt or electric shock. It may be worse when you cough or sneeze, and prolonged sitting also can aggravate symptoms. Usually only one lower extremity is affected.
Sciatica symptoms include:
Pain. It’s especially likely to occur along a path from your low back to your buttock and the back of your thigh and calf.
Numbness or muscle weakness along the nerve pathway in your leg or foot. In some cases, you may have pain in one part of your leg and numbness in another.
Tingling or a pins-and-needles feeling, often in your toes or part of your foot.
A loss of bladder or bowel control. This is a sign of cauda equina syndrome, a rare but serious condition that requires emergency care. If you experience either of these symptoms, seek medical help immediately.
Causes
Sciatica frequently occurs when a nerve root is compressed in your lower (lumbar) spine — often as a result of a herniated disk in your lower back. Disks are pads of cartilage that separate the bones (vertebrae) in your spine. They keep your spine flexible and act as shock absorbers to cushion the vertebrae when you move.
But as you grow older, the disks may start to deteriorate, becoming drier, flatter and more brittle. Eventually, the tough, fibrous outer covering of the disk may develop tiny tears, causing the jelly-like substance in the disk’s center to seep out (herniation or rupture). The herniated disk may then press on a nerve root, causing pain in your back, leg or both. If the damaged disk is in the middle or lower part of your back, you may also experience numbness, tingling or weakness in your buttock, leg or foot.
Although a herniated disk is a common cause of sciatic nerve pain, other conditions also can put pressure on your sciatic nerve, including:
Lumbar spinal stenosis
Spondylolisthesis
Piriformis syndrome
Spinal tumors
Trauma
Sciatic nerve tumor or injury
Treatment
For most people, sciatica responds well to self-care measures. These may include use of hot packs or cold packs, stretching, exercise and use of over-the-counter (OTC) medications. Beyond the self-care measures you may have taken, your doctor may recommend the following:
Physical therapy
Prescription drugs
Epidural steroid injections
Surgery
Prevention
It’s not always possible to prevent sciatica, and the condition may recur. The following suggestions can play a key role in protecting your back:
Exercise regularly
Maintain proper posture
Use good body mechanics
For most people, sciatica responds well to self-care measures. You’ll heal more quickly if you continue with your usual activities, but avoid what may have triggered the pain in the first place. Although resting for a day or so may provide some relief, prolonged bed rest isn’t a good idea. In the long run, inactivity will make your signs and symptoms worse.
11 Wednesday Mar 2015
Posted in car accident, Uncategorized
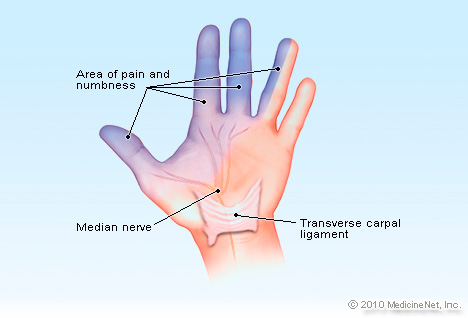
Carpal Tunnel syndrome is a common cause of numbness, pain, and difficulty with movement and strength of the hand caused by pressure and impingement of the median nerve in the wrist.
Carpal Tunnel Syndrome
Carpal tunnel syndrome can be caused by repetitive motion of the wrist or to trauma to the wrist. In either case, the result is entrapment or impingement of the median nerve as it passes through the carpal tunnel in the wrist. It causes numbness or tingling, pain, and weakness of the thumb, index finger, middle finger and half of the fourth finger..
The symptoms are often worse at night. It is believed this is due to flexion of the wrists during sleep. The pain of carpal tunnel syndrome is actually a form of severe numbness that is so severe that it awakens a person from sleep. This has been shown to be the case in electrophysiology studies.
If a patient is not treated or continues to have pain in the affected hand, it can lead to permanent damage to the nerve with atrophy of some of the thumb muscles, and chronic weakness when attempting palmar abduction.
Treatment of carpal tunnel syndrome can be conservative or surgical. Conservative measures include splinting and the injection of corticosteroids. Surgery usually involves cutting the transverse carpal ligament, which frees the nerve from its entrapment.
What is Traumatic Carpal Tunnel Syndrome?
Most people believe that carpal tunnel syndrome is only associated with repetitive stress. It can also be caused by trauma, such as a motor vehicle accident.
Traumatic carpal tunnel syndrome is believed to be caused by shear stress on the wrist that does damage to the ligaments and tendons that surround the median nerve. There aren’t many symptoms in the beginning but, as the tendons and ligaments heal, they form scar tissue that impinges on the nerve, resulting in the classic symptoms of numbness, pain, parasthesias (tingling), and weakness of the part of the hand serviced by the median nerve.
The median nerve travels through the carpal tunnel with nine different tendons and spongy tissue, known as the tenosynovium. If any of the tendons get inflamed, they can pinch the median nerve, causing carpal tunnel. An acute trauma can damage these tendons, leading to subsequent inflammation and scar tissue.
In traumatic carpal tunnel syndrome, the symptoms don’t always show up right away. They can lead to constant or intermittent symptoms of numbness, tingling or pain. The weakness usually is a late finding. Symptoms may be dependent on the activity a patient does such as forming a fist, typing, holding a heavy object, driving, and sleeping.
Because traumatic carpal tunnel syndrome is caused by compression of the median nerve rather than an injury to the median nerve, the symptoms are not immediate. In one study, 6 of 7 patients did not develop symptoms of carpal tunnel syndrome for two weeks up to several months after the traumatic incident. Interestingly, another study showed that approximately 22 percent of people injured in a motor vehicle accident developed CTS.
The fact that the symptoms are delayed leads the doctor to assume that repetitive stress is the cause of the injury and not trauma. The history should be looked at, which will reveal the presence of an incident where the hands were slammed into the dashboard or were gripping the steering wheel. This will lead to the proper diagnosis of traumatically-caused carpal tunnel syndrome.
The diagnosis of traumatic carpal tunnel syndrome is even more complex because there are many other possible causes of similar symptoms. The symptoms can be from a C-spine injury, thoracic outlet syndrome, or compression of nerves at the elbow. A person can, in fact, have multiple diagnoses going on that impact the findings noted in the wrist and hand. If the carpal tunnel aspect of the injuries is not addressed, it could lead to a permanent hand and wrist injury.
Symptoms of Traumatic Carpal Tunnel Syndrome
The major symptoms of traumatic carpal tunnel syndrome include:
A person can have some of these symptoms and not others, depending on how long they have had the disorder.
Causes of Traumatic Carpal Tunnel Syndrome
Traumatic carpal tunnel syndrome is most likely to occur in car accidents. In motor vehicle accidents, the injury is usually caused by front end collisions. In such events, the driver is usually gripping the wheel and can have tendon damage to the forearm from the force of the collision.
Passengers can be injured by falling forward and bracing the collision with their outstretched hands on the dashboard. Depending on where the passenger is sitting, it is possible to have this kind of injury while seat belted. The only way to have some protection for the forearm is to have both passenger and driver-side airbags.
Diagnosis of Traumatic Carpal Tunnel Syndrome
The diagnosis of traumatic carpal tunnel syndrome depends on a history of trauma within the last few months that involved pain or injury to the forearms. It also depends on the presence of the signs and symptoms of carpal tunnel, keeping in mind what is innervated by the median nerve.
One test that is done for the diagnosis of carpal tunnel syndrome is the Tinel’s sign. This is a test where the doctor taps on the median nerve in the wrist. If the patient experiences a sudden “zing” in the hand, the Tinel’s sign is considered to be positive.
The Phalen’s sign is a test where the patient flexes both wrists and puts the backs of the hands together. If the patient has numbness or tingling of the hand when this maneuver is performed, the Phalen’s sign is considered positive for carpal tunnel. In addition, the doctor checks the two point discrimination of the hand to check for numbness.
The doctor can do EMG or electromyography. This involves inserting a tiny needle into the muscles of the arm and hand to see where the nerve is not conducting enough electricity to the muscles. Nerve conduction studies can be done to see which nerves are damaged.
X-rays can check for other problems, such as osteoarthritis, bones that might have been recently broken or any dislocated bones.
Ultrasound can be done to assess the size of the median nerve. It is an inexpensive test; however, its usefulness is as yet unknown. A better test is the MRI, which can detect swelling of the median nerve, narrowing of the carpal tunnel and the possibility of a loss of circulation of the blood through the carpal tunnel.
Blood tests are sometimes performed to see if there are medical conditions leading to carpal tunnel syndrome, including thyroid function studies, a rheumatoid factor or testing for lupus.
Treatment of Carpal Tunnel Syndrome
The idea behind treatment for carpal tunnel syndrome is that treatment can return the patient to normal functioning by reducing inflammation and pressure on the median nerve, and by preventing permanent damage to the nerve. The treatment is based on how severe the condition is and whether or not there is any permanent damage to the nerve.
Many patients do well with nonsurgical treatment, especially if they are being treated early in the course of the disease. Nonsurgical treatment is usually tried first before any surgical intervention is tried.
Nonsurgical treatment includes:
Surgery is sometimes used when all other remedies have not been successful or if there is already damage to the median nerve. During the surgery, the doctor cuts the “roof” off the carpal tunnel by cutting the overlying ligament. This immediately relieves the pressure off of the median nerve and the nerve eventually heals.
This information is compliments of:
WASHINGTON MEDICAL
DR. ROBERT LABACZEWSKI AND DR. DOMINIC LAGANELLA
TO CONTACT OUR OFFICE, PLEASE CALL:
SEWELL AND WOOLWICH TWP: (856) 582-8041
VINELAND: (856) 205-1422
![]()
![]()
|
v\:* {behavior:url(#default#VML);}
o\:* {behavior:url(#default#VML);}
w\:* {behavior:url(#default#VML);}
.shape {behavior:url(#default#VML);}
Normal
0
false
false
false
EN-US
JA
X-NONE
/* Style Definitions */
table.MsoNormalTable
{mso-style-name:”Table Normal”;
mso-tstyle-rowband-size:0;
mso-tstyle-colband-size:0;
mso-style-noshow:yes;
mso-style-priority:99;
mso-style-parent:””;
mso-padding-alt:0in 5.4pt 0in 5.4pt;
mso-para-margin:0in;
mso-para-margin-bottom:.0001pt;
mso-pagination:widow-orphan;
font-size:10.0pt;
font-family:Cambria;}
04 Thursday Dec 2014
Posted in car accident
You’re driving to work with a colleague mindful of the other cars and pedestrians. Suddenly, you’re broad-sided by a speeding car that came our of nowhere…or, stopped at a red light, you are unexpectedly rear-ended by a SUV.
You hit the steering wheel, and your passenger hits the windshield.
Everyone’s first instinct when a motor vehicle accident happens is to ask, “Are you all right?” You check for obvious injuries: Is anyone unconscious? Can you move your arms and legs? Are you or your passenger bleeding?
When no one appears injured, you breathe a sigh of relief: Everyone’s okay.
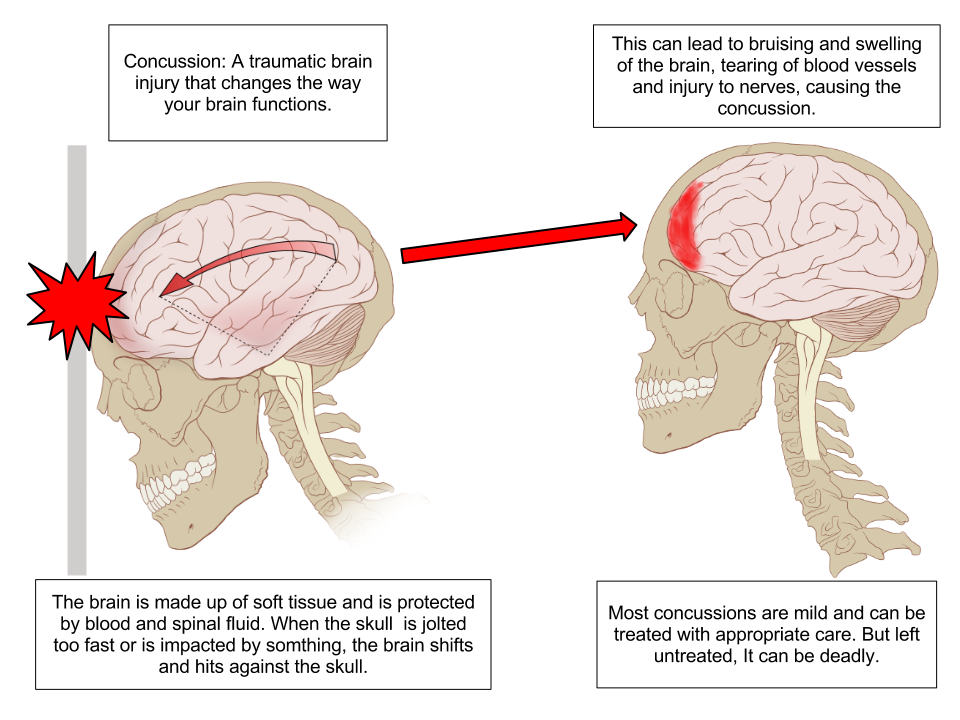
But sometimes everyone is not okay. You or your passenger may have suffered a traumatic brain injury (TBI) that is not obvious, and immediate treatment may make a difference.
In a concussion, the brain is shaken or jostled, but there is no structural injury that can be seen on an X-ray, CT scan or MRI. Yet, after a concussion, the brain isn’t working the way it was prior to the injury. Concussion changes the way a person thinks, acts, sees and functions. An examination by a physician should be performed to evaluate any changes in balance, coordination, reflexes and vision.
You should get medical help immediately if you or anyone else in the accident:
According to the National Institute of Health, you require emergency treatment if you have any of the following symptoms:
It is important to remember that the signs and symptoms of a concussion may not be immediate. Symptoms usually appear within 24 to 72 hours after the injury and can range from mild to severe, lasting for hours, days, weeks or even months.
This information is compliments of:
WASHINGTON MEDICAL
DR. ROBERT LABACZEWSKI AND DR. DOMINIC LAGANELLA
DR. JOHN ASHBY, PMR
EBENEZER OGUNTUASE, PT
TO CONTACT OUR OFFICE,
CALL (856) 582-8041 (SEWELL) OR
(856) 205-1422 (VINELAND)
WWW.WASHINGTONMEDICALPA.COM
ON SITE PHYSICAL THERAPY AND EMG/NVC TESTING
